In the world of counseling, effective communication is key. Have you ever wondered how professionals keep track of client progress and treatment plans? SOAP notes counseling offers a structured approach to documenting sessions that enhances clarity and continuity in care. This method not only streamlines record-keeping but also ensures that essential information is readily accessible for future reference.
Overview of SOAP Notes Counseling
SOAP notes serve as a structured method for documenting client interactions in counseling. This approach enhances communication among professionals and ensures vital information is readily available for future sessions.
Definition of SOAP Notes
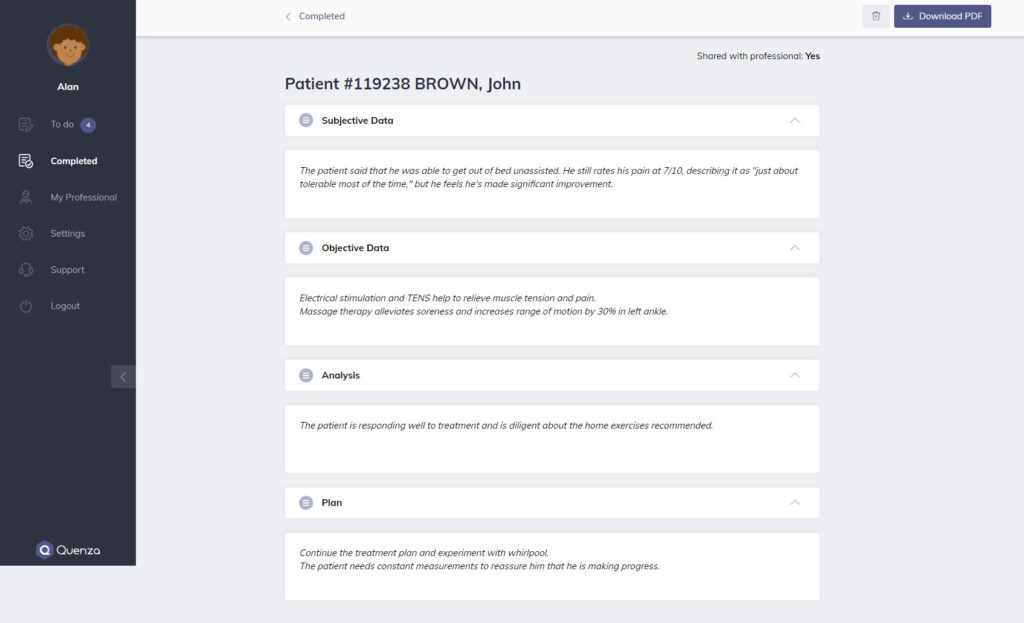
SOAP stands for Subjective, Objective, Assessment, and Plan. Each component plays a crucial role:
- Subjective: Captures the client’s personal experiences and feelings.
- Objective: Documents observable behaviors and factual data.
- Assessment: Provides an analysis based on subjective and objective information.
- Plan: Outlines the next steps or interventions to be taken.
Using this framework helps you maintain clarity in documentation while addressing clients’ unique needs.
Importance in Counseling Practice
Implementing SOAP notes significantly improves your counseling practice. Here’s why:
- Clarity: They offer clear, organized information about each session.
- Continuity of Care: Consistent documentation facilitates understanding across multiple counselors or treatment stages.
- Efficiency: Streamlined records save time during follow-ups or case reviews.
Utilizing SOAP notes promotes effective communication within your team. It ensures everyone remains informed about the client’s progress and treatment strategies.
Components of SOAP Notes
SOAP notes consist of four essential components that help you document counseling sessions effectively. Understanding each part ensures clear communication and continuity in care.
Subjective Section
The Subjective Section captures the client’s personal experiences and feelings. You might include direct quotes or summaries of what the client expresses regarding their thoughts, emotions, or concerns. For example:
- “I feel overwhelmed with work.”
- “I’m having trouble sleeping due to anxiety.”
This section provides context for understanding the client’s perspective and emotional state.
Objective Section
The Objective Section documents observable behaviors and factual information. Here, you can note physical symptoms, non-verbal cues, or relevant data from assessments. Examples include:
- Client appears anxious during sessions.
- Weight loss of 5 pounds since last visit.
Including these details helps create a comprehensive view of the client’s condition based on measurable evidence.
Assessment Section
In the Assessment Section, you analyze the subjective and objective data to formulate a diagnosis or identify issues. This is where you synthesize information gathered so far. For instance:
- Client’s anxiety appears linked to work pressure.
- Symptoms indicate possible adjustment disorder.
Your assessment informs future treatment decisions by summarizing critical insights about the client’s situation.
Plan Section
Finally, the Plan Section outlines next steps for treatment based on your assessment. You should specify interventions, goals, and follow-up actions clearly. Example entries could include:
- Schedule weekly therapy sessions.
- Introduce stress management techniques.
This structured approach ensures everyone involved understands the direction for ongoing care and supports effective collaboration among professionals.
Benefits of Using SOAP Notes in Counseling
Using SOAP notes in counseling provides numerous advantages that enhance the overall effectiveness of treatment.
Improved Documentation
SOAP notes promote systematic documentation. Each session’s details are organized clearly, making it easy for you to track a client’s progress over time. For example, by recording clients’ subjective experiences alongside observable behaviors, you create a holistic view of their situation. This structured approach reduces the risk of overlooking important information.
Enhanced Communication
SOAP notes facilitate better communication among professionals. When different counselors access consistent documentation, they understand the client’s history and treatment plan without needing lengthy explanations. For instance, if one therapist leaves and another takes over, SOAP notes provide essential insights into what has been discussed previously. This transparency fosters collaboration and ensures everyone is on the same page.
Better Continuity of Care
Utilizing SOAP notes strengthens continuity of care. By maintaining clear records, you ensure that all team members can follow the treatment plan effectively. If a client switches therapists or seeks additional support from various providers, these notes allow for seamless transitions in their care. Additionally, obvious connections between sessions help identify patterns or changes in behavior that might require immediate attention.
Challenges in Implementing SOAP Notes
Implementing SOAP notes in counseling faces several challenges that can impact effectiveness. Addressing these obstacles enhances the overall utility of this documentation method.
Time Constraints
Time constraints often hinder effective implementation of SOAP notes. Counselors frequently juggle multiple clients, making it difficult to dedicate enough time to detailed documentation. For example, a session may end just before another appointment begins, leaving little room for thorough note-taking. To improve documentation efficiency:
- Prioritize concise entries while capturing essential information.
- Use templates to streamline the writing process.
- Schedule dedicated time after sessions for comprehensive note completion.
Consistency in Documentation
Consistency in documentation poses another challenge with SOAP notes. Variability among counselors’ approaches may lead to incomplete or inconsistent records. This inconsistency can obscure vital client information and disrupt continuity of care. Striving for uniformity involves:
- Establishing clear guidelines on what each section should include.
- Conducting regular reviews of completed notes for adherence to standards.
- Offering feedback and training sessions to ensure all team members follow best practices.
Training and Education Needs
Training and education needs significantly affect the successful implementation of SOAP notes. Without proper understanding, counselors might struggle with effectively using this framework. For instance, new professionals may require instruction on how to accurately capture subjective experiences or objective observations. To address these educational gaps:
- Provide workshops focusing on each component of SOAP notes.
- Develop online resources or manuals for ongoing reference.
- Encourage mentorship programs where experienced practitioners guide novices through the process.
By tackling these challenges head-on, you enhance your practice’s use of SOAP notes and ultimately support better client outcomes.